
Modulnavigering
Denne modulen inneholder enkle navigasjonsverktøy som hjelper deg med å finne frem. Her er noen ikoner du bør se etter:
Generell navigasjon
Interaktive elementer
Frem og tilbake for å se gjennom bildene
Dra til siden
Klikk for neste
Bruk plussikonet til å åpne popup-vinduer med tilleggsinformasjon
Klikk for neste visning
Lukk popup-vinduer for å gå tilbake til hovedbildet
Skift mellom visninger
Klikk for mer informasjon
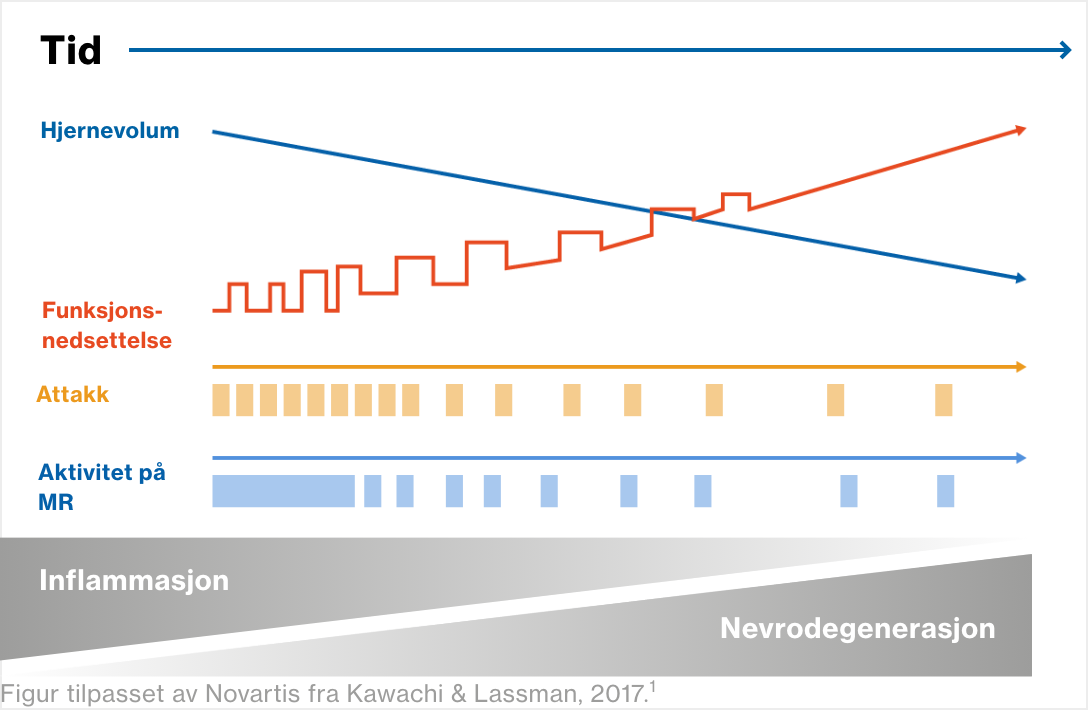
Å gjenkjenne aktivitet/progresjon
Multippel sklerose er en autoimmun sykdom som rammer sentralnervesystemet og forårsaker akkumulerende funksjonsnedsettelse1
I begynnelsen forekommer det mest inflammasjon, men over tid oppstår det mer nevrodegenerasjon1.2
og økt funksjonsnedsettelse uavhengig av akutte attakk (tilbakefall eller forverringer).3
For mer informasjon om hvordan akkumulerende funksjonsnedsettelse vurderes klinisk, se senere bilder i denne modulen og se modul 3: Vurdering av MS-pasienter.
Lesjoner i hjerne og ryggmarg samt tap av hjernevolum (atrofi) kan ses på MR-undersøkelser (magnetresonanstomografi). For mer informasjon, se senere bilder i denne modulen, og se modul 3: Vurdering av MS-pasienter.

Referanser
- Kawachi I, Lassmann H. Neurodegeneration in multiple sclerosis and neuromyelitis optica. J Neurol Neurosurg Psychiatry. 2017;88:137–145.
- Dobson R, Giovannoni G. Multiple sclerosis – a review. Eur J Neurol. 2019;26:27–40.
- Scalfari A, et al. The natural history of multiple sclerosis, a geographically based study 10: relapses and long-term disability. Brain. 2010:133;1914–1929.
Å gjenkjenne aktivitet/progresjon
MS kan være aktiv i alle stadier, uavhengig av progresjon, også før diagnose1,2
Tegn på tidlig sykdomsaktivitet er sett hos personer som ennå ikke har fått en MS-diagnose, men som har radiologisk isolert syndrom (RIS) eller klinisk isolert syndrom (CIS).
Bekreftet MS kan være aktiv i alle stadier, uavhengig av sykdomsprogresjon / progresjon av funksjonsnedsettelse.
Dette er MS-undertypene, ofte kalt 2013-klassifiseringen.1 Klikk på de blå boksene for fiktive kasushistorier
RRMS – Ikke aktiv3
Anne er 24 år gammel og ble henvist til nevrolog for mer enn syv år siden med en historie med migrene. MR-bildene viste en unormal endring i hvit substans som var periventrikulær. Ett år senere rapporterte hun om nedsatt syn ledsaget av øyesmerter (høyre øye) i fem dager, og seks måneder etter dette hadde hun en firedagers episode med svakhet i venstre ben. Begge de akutte anfallene gikk over ved hjelp av intravenøs metylprednisolon. Hun har ikke hatt noen ytterligere attakk de siste seks årene. I løpet av denne perioden har de årlige MR-undersøkelsene ikke vist nye MS-lesjoner, og det har ikke vært noen klinisk progresjon verken ved fysiske undersøkelser eller selvrapportering.
Referanser
- Lublin FD, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83:278–286.
- Klineova S, Lublin FD. Clinical course of multiple sclerosis. Cold Spring Harb Perspect Med. 2018;8:a028928.
- Pasientkasus: Illustrative fictional case.
Å gjenkjenne aktivitet/progresjon
MS-behandling har som mål å beskytte den nevrologiske reserven1,2


Referanser
- Giovannoni G, et al. Brain health: time matters in multiple sclerosis. Mult Scler Relat Disord. 2016;9 Suppl 1:S5–S48.
- Leino-Kilpi, Helena et.al. Elements of Empowerment and MS Patients. Journal of Neuroscience Nursing, vol.30, no.2, Apr. 1998 pp.116+
Å gjenkjenne aktivitet/progresjon
Tidlig intervensjon med sykdomsmodifiserende terapier (DMT) er viktig.1-5



Figur tilpasset av Novartis fra Giovannoni G, et al. Mult Scler Rel Disord 2016:9:S5‒S8
Referanser
- Giovannoni G, et al. Brain health: time matters in multiple sclerosis. Mult Scler Rel Disord. 2016:9:S5‒S8.
- Rocca MA, et al. Evidence for axonal pathology and adaptive cortical reorganization in patients at presentation with clinically isolated syndromes suggestive of multiple sclerosis. Neuroimage 2003;18:847–855.
- De Stefano N, et al. Assessing brain atrophy rates in a large population of untreated multiple sclerosis subtypes. Neurology. 2010;74:1868–1876.
- Merkel B, et al. Timing of high-efficacy therapy in relapsing-remitting multiple sclerosis: a systematic review. Autoimmun Rev. 2017;16:658–665.
- Brown JWL, et al. Association of initial disease-modifying therapy with later conversion to secondary progressive multiple sclerosis [published correction appears in JAMA. 2020:7;323:1318]. JAMA. 2019;321:175–187.
Patofysiologi
Flere patologiske prosesser bidrar til nevrodegenerasjon
Autoimmune prosesser forårsaker patologiske endringer i CNS. Inflammasjon starter tidlig i sykdomsforløpet:

Til slutt fører progressivt tap av demyeliniserte aksoner til akselerert tap av hjernevev ‒ hjerneatrofi.4


Figur utarbeidet av Novartis på bakgrunn av Chari DM. Remyelination in multiple sclerosis. Int Rev Neurobiol. 2007;79:589–6202
Referanser
- Joy JE, Johnston RB Jr., editors. Multiple Sclerosis: Current Status and Strategies for the Future. Washington (DC): National Academies Press (US); 2001: pp. 43, 60.
- Chari DM. Remyelination in multiple sclerosis. Int Rev Neurobiol. 2007;79:589–620.
- Oh J, et al. Diagnosis and management of secondary-progressive multiple sclerosis: time for change. Neurodegener Dis Manag. 2019;9:301–317.
- Wang C, et al. Lesion activity and chronic demyelination are the major determinants of brain atrophy in MS. Neurol Neuroimmunol Neuroinflamm. 2019;6:e5933.
- Joy JE, Johnston RB Jr., editors. Multiple Sclerosis: Current Status and Strategies for the Future. Washington (DC): National Academies Press (US); 2001: pp. 43, 56, 57, 60, 243.
Patofysiologi
PPMS

PPMS
Aktive lesjoner er sjeldne2
Hjerneatrofi er vanlig2
Mindre inflammasjon enn ved RRMS3
Lesjoner som blir større over tid2
Aktivitering av mikrogliale celler (immunceller i CNS) i normal grå og hvit substans er fremtredende2
Der er lesjoner i hjernen og ryggmargen, men i motsetning til RRMS er der mer sannsynlig at de er begrenset til ryggmargen4
RRMS

RRMS
Aktivt demyeliniserende plakk er den mest fremtredende typen lesjon2
Flere nye hjernelesjoner (plakk) enn ved PPMS5
Lesjoner av typen inflammatorisk demyelinering, 2 og flere inflammatoriske lesjoner enn ved PPMS,3,5
Aksonal transseksjon (brudd på axoner) er vanlig2
Det er lesjoner i hjernen og ryggmargen, men i motsetning til PPMS er det mer sannsynlig at de er begrenset til hjernen4
SPMS

SPMS
Hjerneatrofi i grå substans spiller en sentral rolle i progresjon av funksjonsnedsettelse, og driver irreversibel akkumulering av funksjonsnedsettelse6,7 og bidrar til kognitiv svikt8
Referanser
- Kanavos P, et al. Towards better outcomes in multiple sclerosis by addressing policy change: The International MultiPlE Sclerosis Study (IMPrESS). 2016. Available at: http://www.lse.ac.uk/business-and-consultancy/consulting/consulting-reports/towards-better-outcomes-in-ms. Accessed: January 2021.
- Macaron G, Ontaneda D. Diagnosis and management of progressive multiple sclerosis. Biomedicines. 2019;7:56.
- National Multiple Sclerosis Society. (A) Primary Progressive MS. Available at: https://www.nationalmssociety.org/What-is-MS/Types-of-MS/Primary-progressive-MS. Accessed: January 2021.
- Dastagir A, et al. Brain and spinal cord MRI lesions in primary progressive vs. relapsing-remitting multiple sclerosis. eNeurologicalSci. 2018;12:42–46.
- National Multiple Sclerosis Society (B). Relapsing Remitting MS. Available at: https://www.nationalmssociety.org/What-is-MS/Types-of-MS/relapsing-remitting-MS. Accessed: January 2021.
- Fisher E, Lee JC, Nakamura K, Rudick RA. Gray matter atrophy in multiple sclerosis: a longitudinal study. Ann Neurol. 2008;64:255–265.
- Calabrese M, et al. The changing clinical course of multiple sclerosis: a matter of gray matter. Ann Neurol. 2013;74:76–83.
- Amato MP, et al. Association of neocortical volume changes with cognitive deterioration in relapsing-remitting multiple sclerosis. Arch Neurol. 2007;64:1157–1161.
Tegn og symptomer på progresjon
Progresjon kan omfatte mange symptomer og er ulik fra pasient til pasient1-6







Du finner mer informasjon om symptomer og hvordan de vurderes og behandles i modul 2 til 5.
Referanser
- Scalfari A, et al. Onset of secondary progressive phase and long-term evolution of multiple sclerosis. J Neurol Neurosurg Psychiatry 2014;85:67‒75.
- National MS Society (NMSS). Multiple Sclerosis: Just the Facts. NMSS; 2018 Available at https://www.nationalmssociety.org/nationalmssociety/media/msnationalfiles/brochures/brochure-just-the-facts.pdf. Accessed: December 2020.
- Papathanasiou A, et al. Cognitive impairment in relapsing remitting and secondary progressive multiple sclerosis patients: efficacy of a computerized cognitive screening battery. ISRN Neurol. 2014;2014:151379.
- Gross HJ, Watson C. Characteristics, burden of illness, and physical functioning of patients with relapsing-remitting and secondary progressive multiple sclerosis: a cross-sectional US survey. Neuropsychiatr Dis Treat. 2017;13:1349–1357.
- Beiske AG, et al; Nordic SPMS study group. Health-related quality of life in secondary progressive multiple sclerosis. Mult Scler. 2007;13:386‒392.
- Ziemssen T, et al. A mixed methods approach towards understanding key disease characteristics associated with the progression from RRMS to SPMS: Physicians’ and patients’ views. Mult Scler Relat Disord. 2020;38:101861.
Screeningsverktøy
Screeningsverktøy som evaluerer flere symptomer, kan bidra til å følge opp progresjon av funksjonsnedsettelse over tid
En signifikant utfordring når man skal overvåke progresjon ved MS, er vanskeligheter med å kvantifisere funksjonsnedsettelse over tid.1 Eksempler på screeningverktøy er:



Referanser
- Ontaneda D, Fox RJ. Progressive multiple sclerosis. Curr Opin Neurol. 2015;28:237–243.
- Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33:1444–1452.
- Fischer JS, et al. Multiple Sclerosis Functional Composite (MSFC). Administration and Scoring Manual. New York: National Multiple Sclerosis Society, 2001. Available at: https://www.nationalmssociety.org/NationalMSSociety/media/MSNationalFiles/Brochures/10-2-3-31-MSFC_Manual_and_Forms.pdf.
- Thompson H, Mauk KL (Eds). Nursing management of the patient with multiple sclerosis. AANN and ARN Clinical Practice Guideline Series, 2011. Available at: http://iomsn.org/wp-content/uploads/2016/07/AANN-ARN-IOMSN-MS-Guideline_FINAL.pdf. Accessed: September 2020.
Oppfølging av attakker (1/3)
Attakk indikerer underliggende sykdomsaktivitet og kan forutsi progresjon av funksjonsnedsettelse1
Et attakk er en forbigående klinisk episode av sykdomsaktivitet som innebærer inflammasjon og/eller aktiv demyelinisering:2
Manglende bedring etter attakker ved RRMS er forbundet med kortere tid til progresjon til SPMS3
Attakker før og etter progresjon akselererer tiden til alvorlig funksjonsnedsettelse (EDSS 6) ved progressiv MS4
Selv om de fleste attakker etterfølges av klinisk remisjon, kan noen symptomer vedvare og bidra til progresjon av funksjonsnedsettelse5

Figur tilpasset av Novartis fra Soldán MMP, et al. Neurology 2015;84:81–88.4
Referanser
- Giovannoni G, et al. Brain health: time matters in multiple sclerosis. Mult Scler Rel Disord 2016:9:S5‒S8.
- Kalincik T. Multiple sclerosis relapses: epidemiology, outcomes and management. A systematic review. Neuroepidemiology 2015;44:199–214.
- Novotna M, et al. Poor early relapse recovery affects onset of progressive disease course in multiple sclerosis [published correction appears in Neurology. 2015 Oct 13;85:1355]. Neurology. 2015;85:722–729.
- Soldán MMP, et al. Relapses and disability accumulation in progressive multiple sclerosis. Neurology. 2015;84:81–88.
- Leray E, et al. Evidence for a two-stage disability progression in multiple sclerosis. Brain. 2010;133:1900–13.
Magnetresonanstomografi (MR) (1/8)
MR-oppfølging sørger for bevis på aktiv sykdom
Fokale lesjoner på MR er det patologiske kjennetegnet på MS1 som forekommer i hjernen og ryggmargen:1,2
Hjerne-MR er abnormal hos nesten alle personer med etablert MS og
80 % av de som har CIS2Lesjoner i ryggmargen forekommer hos >80 % av personer med etablert MS og opptil 50 % av personer med CIS (vanligvis cervikalt)2
Nye hjernelesjoner oppdages 10 ganger oftere enn attakk oppstår,3 noe som gjør at hjerne-MR er svært følsom for overvåking av sykdomsaktivitet.4 I tillegg kan lesjonsbelastning brukes som en prediktor for langsiktig progresjon av funksjonsnedsettelse4

Referanser
- Sastre-Garriga J, et al. MAGNIMS consensus recommendations on the use of brain and spinal cord atrophy measures in clinical practice. Nat Rev Neurol. 2020;16:171–182.
- Brownlee WJ, et al. The diagnosis and differential diagnosis of multiple sclerosis: progress and challenges. Lancet. 2017; 389: 1336–1346.
- Dobson R, Giovannoni G. Multiple sclerosis – a review. Eur J Neurol. 2019;26:27–40.
- Wattjes MP, et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis – establishing disease prognosis and monitoring patients. Nat Rev Neurol. 2015;11:597–606.
- Lublin FD, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83:278–286
Snakke om progresjon
Sykepleiere spiller en viktig rolle når det gjelder å snakke om progresjon
Sykepleiere spiller en viktig rolle når det gjelder å gi støtte til pasienter og deres omsorgspersoner i forbindelse med diagnostisering av SPMS ved å sørge for:1
Opplæring
Oppmuntring
Psykososial støtte og støtte av egenbehandling
En motvekt til misoppfatninger knyttet til SPMS og behandling av denne formen for MS
Diskusjon om aktiv vs. inaktiv sykdom kan få betydning her fordi det har innvirkning på DMT-behandling.

Referanser
- Oh J, et al. Diagnosis and management of secondary-progressive multiple sclerosis: time for change. Neurodegener Dis Manag. 2019;9:301–317.
Kunnskapstest
Test din viten nedenfor
